

A. INCIDENT (Verbatim per MB Lal Repor)
1.1 In the evening shift of October 29, 2009, the Indian Oil Corporation (Petroleum Oil and Lubricants) Terminal at Sanganer in Jaipur, India was preparing to transfer Motor Sprit to the neighbouring BPCL terminal a routine operation.
1.2. In the process of lining up the MS tank 401A at about 6.10 PM, a huge leak of MS (Gasoline) took place as a jet of liquid from the Hammer Blind on the delivery line of the Tank leading to the MS pump.
1.3. The liquid MS which rapidly generated vapours soon overwhelmed and incapacitated the operator carrying out the line-up operation. The shift officer, who was nearby, tried to help the operator, but he was affected by the vapours and the liquid and had to be moved to hospital in semi-conscious state. The 2nd operator who was incidentally into the canteen at the time, also rushed to the spot but he was also completely overpowered by the strong vapours and liquid and could not be rescued. The 3rd operator on the shift who was supposed to be on site had earlier left for home on some personal work and thus was not available to initiate any rescue or mitigative steps.
1.4.With none of the operating crew being available any more for initiating control actions, the leak continued unabated and by the time the senior staff and civil authorities could reach the site, it had already engulfed almost the entire installation making their entry not only difficult but dangerous.
1.5. After about an hour and 15 minutes (75 minutes) of the leak started, there was a massive explosion followed by a huge fireball covering the entire installations. It is estimated that in this one hour and 15 or 20 minutes of uncontrolled leak about 1000 tons of MS could have escaped out which could have generated enough vapour to cause an explosion with a equivalence of 20 Tons of TNT. The source of ignition, which triggered explosion and fire could be from one of the non- flame proof equipment in the Administrative Block, or from the vehicle being started in the installation.
B. Preamble:
For Jaipur Terminal Fire and Explosion pre and post hazardous events mapping study and analysis have been done in this paper. Since PHAST software during 2009 did not have the facility of Consequence modelling of Motor Spirit therefore the PHAST calculations based Hexane as the MS have been done on conservative basis. These consequence results are compared with the manual calculations using MS as the hazardous fluid. Although Main Accident Hazard had occurred 75 minutes after the start of leak from 250 mm dia. piping from the MS Tank, however other hazards had started soon after 30 minutes of the leak and continued for 11 days. This report accounts for these events. Although the main focus is on MAH after 75 minutes of the MS leak; but the pre and post MAH events described in the report give important information about the incapacitation of operators exposed to the MS vapours before MAH as well as inadequacies of the control and safety systems to handle the Emergency before and after MAH.
Note: The MS leakage, MS evaporated and TNT numbers as given in M.B. Lal report cannot be verified as perhaps based on different basis, although are at variance from the author’s calculations from both methods later Para F.1 and Para F.2 and the actual plot plan of the Terminal with area 110 hectares.
C. Process Description of MAH:
The POL installation receives liquid petroleum products, stores them and despatches these products through pipeline and Tank Lorries. The MS Tank (TK 401A,15 m high and 24 m diameter) involved in the MAH has an inlet piping system equipped with MOV also has an outlet piping connected to a pump with 10’’ MOV followed by a Hammer Blind and HOV of same diameter in the line-up as depicted in the following diagram. During the time of MAH, initial level of the tank is assumed 9 m.
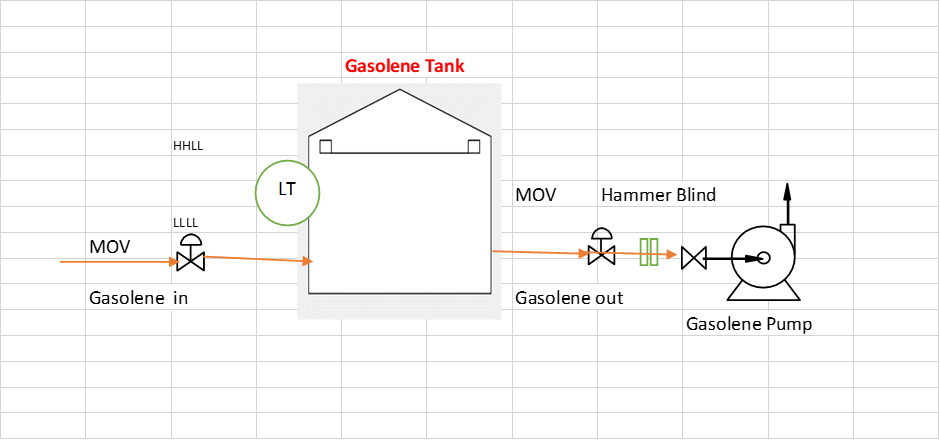
Instrumentation and Controls of the TK401A System
TK 401A had a LIT indicating level in the tank and HHLL triggering closure of inlet MOV and LLLL triggering tripping of Gasoline pump. MOV on the tank discharge line was to close either at remote panel or locally. It is understood that since 2003, this MOV’s remote operation was not working as a result it can be closed either from local closing Push Button arrangement or manually throu
D. Mis-operation causing MAH on TK401A at 6.10 pm of 29 October 2009.
During the tank line up to Gasoline pump following desired operations vs actually operations were done are compared in the following Table:
| Operation should have been done | Operation actually done | Result of the wrong operation | Troubleshooting not done due to site conditions or some other problems |
| 1.Open HOV at the discharge of the tank | 1.Inadvertently Opened MOV | MS started leaking | Closure of MOV from remote panel was not possible as defunct since 2003.Closure of MOV from site was not possible as operating staff were incapacitated by MS vapours |
| 2.Switch Hammer Blind to Open Position | 2.Switched Hammer Blind to Open position | MS started leaking | Switch Hammer Blind to close position was not possible as MS pressure was higher in the piping |
| 3. Slowly open MOV | 3.HOV could not be opened | The pressure in the piping was higher | HOV could not be opened as pressure in the piping was higher and MS was leaking as fountain. |
E. Before MAH Scenario :
Leak started at 6.10 PM and 20 minutes thereafter (till @ 6.30 pm) about 557 Tons of MS was released from the tank TK401A with evaporation of MS of about 27.9 tons and balance MS making MS pool on the tank dyke. The MS vapours in the surrounding air has a volume of 6884 m3 surpassing IDLH limits and therefore the operators on the ground died. It is important to mention that there was no SCBA available for the persons working in the area. The Shift Officer who climbed on the Tank (15 m from the ground), was beyond MS vapour cloud, was only partially exposed to MS vapours and could be shifted to hospital in semiconscious conditions. But this action of Shift Officer cannot be called safe because in the post Fire Scenario the tank has collapsed and if he were on the tank top he would have died. It was his luck that he climbed down from the tank in time to the ground and in semiconscious state was shifted to the hospital.
F. Main MAH Scenario:
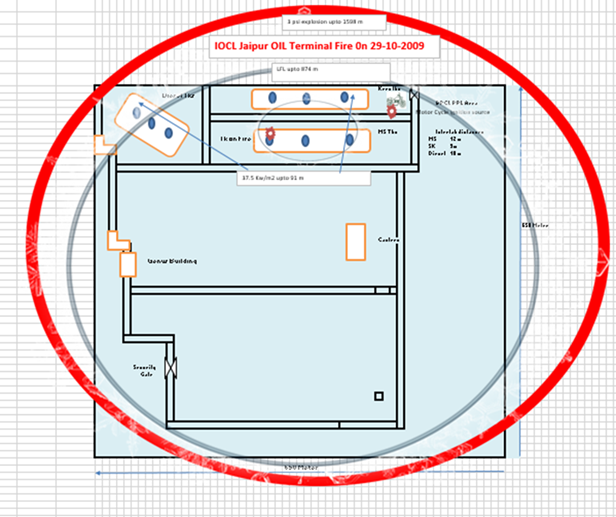
As per Para F.1, see later, 275 minutes after the leak (till about 7.35 pm) about 2091879 Tons of MS was released from the tank with evaporation of MS of about 199495 tons to air and balance MS making pool. The MS vapours in the surrounding air has a volume of 2485242 Nm3 of vapour cloud (in the flammable range) ,considering about 3 meter height of the cloud it could be square of 910 mX910 m. The area of POL terminal is 110 acre i.e. 667mX667 m. It means that the MS vapours had gone outside of the terminal too. Outside an ignition source of a bike ignited the vapour cloud and fire followed by explosion took place. Ignition source from within the terminal is ruled out as had it been the case the fire should have started much earlier than 7.35 pm.
This MAH scenario has been simulated through Manual Calculations in Para F.1 and with PHAST Para F.2.
F.1:For Manual Analysis with MS and 1 hour 30 MS leak the following Consequence parameters have been calculated:
Release from Tank in 75 minutes: 2091879 Kg
Flammable mass in vapour cloud: 199495 kg
| Wind condition | Flammable mass | Used Flammable mass | Ignition source | Cloud Front Centre |
| 1.5 F | 199495kg | 199495 kg | ||
| Late Explosion Results | ||||
| 0.2 Bar | 0.34 Bar | 0.57 Bar | ||
| 1.5 F | 1100m | 800m | 600 m | |
| Flash Fire | ||||
| LFL | LFL fraction | |||
| 1.5F | 800 m | |||
F.2: For PHAST Analysis with MS as Hexane and 1 hour MS leak the following Consequence parameters have been calculated:
| Wind condition | Flammable mass | Used Flammable mass | Ignition source | Cloud Front Centre |
| 1.5 F | 221105 | 221105 | 1100m | 1100 m |
| Late Explosion Results | ||||
| 1 psi (0.0268 Bar) | 2 psi (0.1379 Bar | 3 psi (0.208Bar) | ||
| 1.5 F | 3588 m | 1744 m | 1598 m | |
| Flash Fire | ||||
| LFL | ||||
| 874m | ||||
| Late Pool Fire | ||||
| Pool Dia | 4 kw/m2 | 12.5 Kw/m2 | 37.5 Kw/m2 | |
| 1.5F | 461 m | 451m | 241 m | n/a |
| Leak | ||||
| UFL | LFL | |||
| 34 m | 874 m | |||
Comparison of results of Para F.1 and Para F.2 is given in with the following Table:
| Wind condition | Flammable mass | Used Flammable mass | Ignition source | Cloud Front Centre |
| 1.5F, Para F.1 | 199495kg | 199495 kg | ||
| 1.5 F ,Para F.2 | 221105kg | 221105 kg | 1000 m | 1000 m |
| Late Explosion Results | ||||
| 0.2 Bar(3psi) | 0.34 Bar | 0.57 Bar | ||
| 1.5 F, Para F.1 | 1100m | 800m | 600 m | |
| 1.5F, Para F.2 | 1598,m | n/a | n/a | |
| Flash Fire | LFL | |||
| 1.5F ,Para F.1 | 800 m | |||
| 1.5 F, Para F.2 | 874 | |||
| Pool Fire | ||||
| Pool Dia | ||||
| 1.5F, Para F.1 | 45 m | |||
| 1.5 F , Para F.2 | 77 m | |||
These results are plotted on the plot plan of the Jaipur Terminal on the next page.
G. Weaknesses of the Jaipur MS Storage and Despatch System:
G.1 Inherent Safety in Design (ISD)
G.1.1 Isolation:
G.1.1.1 MOV should have been equipped with a manual override or guard for operation. This feature allows the valve to be operated manually, bypassing the motorized actuator, in situations like power failures or when the automatic system malfunctions. It was missing in this case
G.1.1.2 MOV on a tank often has a manual isolation valve, also known as a root valve. This manual valve provides a backup or emergency means to isolate the tank if the motorized valve fails or needs to be shut down manually. It was not considered in ISD.
G.1. 1.3 Inter-tank distance as given did not consider consequence of vapour leak, fire and domino effect, therefore damage did occur to adjacent MS tanks along with serious damage to MS401A tank involved in MAH.
G.1.1.4 Inter Tank Transfer Facility was not considered in the design so tank to tank transfer could not be done.
G.2 Preventive Barriers
G.2.1 There was no Flammable Gas Detectors to forewarn the operators of imminent danger of Flammable gas leak of alarming level in the area near MS tanks.
G.2.2 There was no Emergency Shutdown facility to leave the MOV in Closed state during the flammable Gas leak Detection.
G.3 Recovery Barriers
G.3.1 There was no PA/GA communication System on the site connected to F&G panel linked to Flammable Gas Detectors.
G.3.2 Fire Water system and /or Foam System was not charged perhaps due to non-availability of Fire Operators. This was a serious lapse.
G.4 Process Safety Management System
G.4.1 The operators and Shift Officer did not have any knowledge of likelihood of human failure which caused the mal operation and MAH.
G.4.2 Process Safety Management was substandard due to which strategies of tackling MAH scenario were missing.
H. Recommendations
H.1 Recommendations given by MB LAL Committee are good for all such installations and must be implemented.
H.2 Based on author’s experience unless Indian refineries adopt ‘’Process Safety” as concept rather safety indicators based on ‘’Lost Time Hours’’ concept, there are chances of many slippages in the journey of Safety.
For any comments, query or clarifications, please contact:
Krishn Kumar Bhatnagar
Process Safety and Process Consultant